Medtronic Evolut™ TAVR
Valve design makes a difference.
From day one, this valve was designed specifically for transcatheter AVR with performance as the driving force.
 Indications, Safety, and Warnings
Indications, Safety, and Warnings
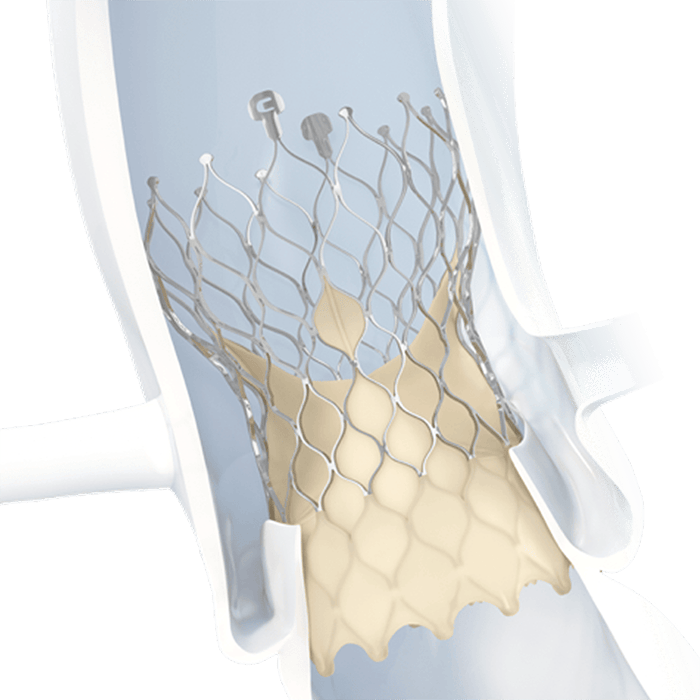
Supra-annular valve: keeps functional portion of the valve above the annulus for lower gradients and reduced workload on the left ventricle.3,4

External tissue wrap: increases surface contact with native anatomy, providing advanced sealing.5

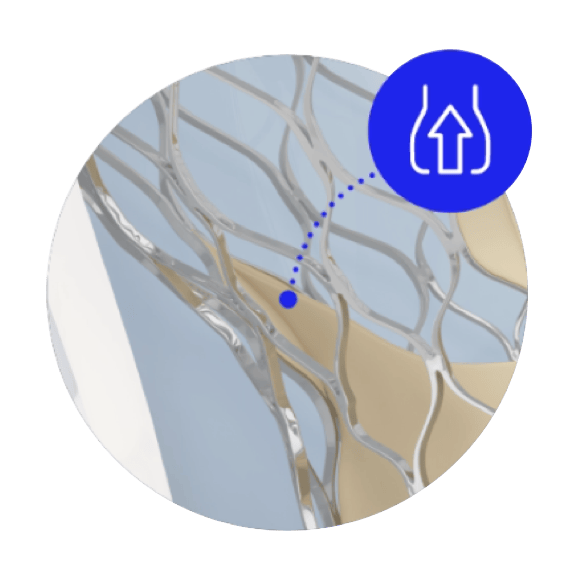
Larger frame windows: four times larger windows to enable lifetime management solutions such as coronary access.6
Because women typically have smaller annuli than men, they require a valve that provides the largest area of blood flow to maximize valve performance.‡,7
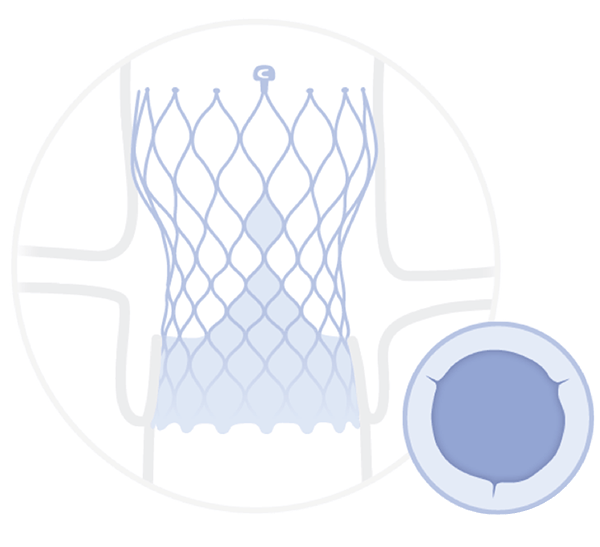
Supra-annular |More Room3
Intra-annular |Less Room3
‡ Valve performance as defined as freedom from bioprosthetic valve dysfunction (BVD) through 12 months. BVD is defined as a composite including any of the following: hemodynamic structural valve dysfunction (mean gradient ≥ 20 mmHg), non-structural valve dysfunction (severe prothesis-patient mismatch or ≥ moderate aortic regurgitation), clinical thrombosis, endocarditis, and aortic valve reintervention.
™* Third-party brands are trademarks of their respective owners. All other brands are trademarks of a Medtronic company.
UC202600896 EN 06/2025